Pulmonology
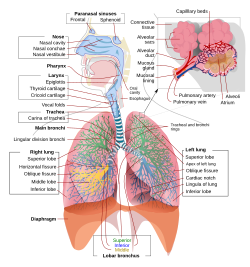 Schematic view of the human respiratory system with their parts and functions. | |
| System | Respiratory |
|---|---|
| Significant diseases | Asthma, Lung Cancer, Tuberculosis, Occupational lung disease |
| Significant tests | Bronchoscopy, Sputum studies, Arterial blood gases |
| Specialist | Respiratory Physician, Pulmonologist |
Pulmonology is a medical speciality that deals with diseases involving the respiratory tract.[1] The term is derived from the Latin word pulmō, pulmōnis ("lung") and the Greek suffix -λογία, -logia ("study of"). Pulmonology is synonymous with pneumology (from Greek πνεύμων ("lung") and -λογία), respirology and respiratory medicine.
Pulmonology is known as chest medicine and respiratory medicine in some countries and areas. Pulmonology is considered a branch of internal medicine, and is related to intensive care medicine. Pulmonology often involves managing patients who need life support and mechanical ventilation. Pulmonologists are specially trained in diseases and conditions of the chest, particularly pneumonia, asthma, tuberculosis, emphysema, and complicated chest infections. [2]
Contents
1 Variations in nomenclature
2 Diagnosis
3 Procedures
3.1 Surgical procedures
4 Treatment and therapeutics
5 Education and training
5.1 Pediatric pulmonologist
6 Scientific research
7 Journals of pulmonology
8 History of pulmonology
9 References
Variations in nomenclature
In the United Kingdom, the term "respiratory physiologist" is used[3]. In Ireland, South Africa[dubious ], and Australia the term "respiratory physician" is used (rather than pulmonologist) to distinguish a physician that practices pulmonology. In Canada, respirology and respirologist are used [1]. Surgery of the respiratory tract is generally performed by specialists in cardiothoracic surgery (or thoracic surgery), though minor procedures may be performed by pulmonologists. As mentioned above, pulmonology is closely related to critical care medicine when dealing with patients who require mechanical ventilation. As a result, many pulmonologists are certified to practice critical care medicine in addition to pulmonary medicine. There are fellowship programs that allow physicians to become board certified in pulmonary and critical care medicine simultaneously. Interventional pulmonology is a relatively new field within pulmonary medicine that deals with the use of procedures such as bronchoscopy and pleuroscopy to treat several pulmonary diseases. Interventional pulmonology is increasingly recognized as a specific medical specialty.[4]
Diagnosis
The pulmonologist begins the diagnostic process with a general review focusing on:
hereditary diseases affecting the lungs (cystic fibrosis, alpha 1-antitrypsin deficiency)- exposure to toxins (tobacco smoke, asbestos, exhaust fumes, coal mining fumes)
- exposure to infectious agents (certain types of birds, malt processing)
- an autoimmune diathesis that might predispose to certain conditions (pulmonary fibrosis, pulmonary hypertension)
Physical diagnostics are as important as in the other fields of medicine.
- Inspection of the hands for signs of cyanosis or clubbing, chest wall, and respiratory rate.
- Palpation of the cervical lymph nodes, trachea and chest wall movement.
Percussion of the lung fields for dullness or hyper-resonance.
Auscultation (with a stethoscope) of the lung fields for diminished or unusual breath sounds.
Rales or rhonchi heard over lung fields with a stethoscope.
As many heart diseases can give pulmonary signs, a thorough cardiac investigation is usually included.
Procedures
Laboratory investigation of blood (blood tests). Sometimes arterial blood gas measurements are also required.
Spirometry the determination of maximum airflow at a given lung volume as measured by breathing into a dedicated machine; this is the key test to diagnose airflow obstruction.
Pulmonary Function Tests spirometry, as above, plus response to bronchodilators, lung volumes, and diffusion capacity, the latter a measure of lung oxygen absorptive area
Bronchoscopy with bronchoalveolar lavage (BAL), endobronchial and transbronchial biopsy and epithelial brushing- Chest X-rays
- CT scanning
Scintigraphy and other methods of nuclear medicine
Positron emission tomography (especially in lung cancer)
Polysomnography (sleep studies) commonly used for the diagnosis of Sleep apnea
Surgical procedures
Major surgical procedures on the heart and lungs are performed by a thoracic surgeon. Pulmonologists often perform specialized procedures to get samples from the inside of the chest or inside of the lung. They use radiographic techniques to view vasculature of the lungs and heart to assist with diagnosis.
Treatment and therapeutics
Medication is the most important treatment of most diseases of pulmonology, either by inhalation (bronchodilators and steroids) or in oral form (antibiotics, leukotriene antagonists). A common example being the usage of inhalers in the treatment of inflammatory lung conditions such as asthma or chronic obstructive pulmonary disease. Oxygen therapy is often necessary in severe respiratory disease (emphysema and pulmonary fibrosis). When this is insufficient, the patient might require mechanical ventilation.
Pulmonary rehabilitation has been defined as a multidimensional continuum of services directed to persons with pulmonary disease and their families, usually by an interdisciplinary team of specialists, with the goal of achieving and maintaining the individual's maximum level of independence and functioning in the community. Pulmonary rehabilitation is intended to educate the patient, the family, and improve the overall quality of life and prognosis for the patient. Interventions can include exercise, education, emotional support, oxygen, noninvasive mechanical ventilation, optimization of airway secretion clearance, promoting compliance with medical care to reduce numbers of exacerbations and hospitalizations, and returning to work and/or a more active and emotionally satisfying life. These goals are appropriate for any patients with diminished respiratory reserve whether due to obstructive or intrinsic pulmonary diseases (oxygenation impairment) or neuromuscular weakness (ventilatory impairment). A pulmonary rehabilitation team may include a rehabilitation physician, a pulmonary medicine specialist, and allied health professionals including a rehabilitation nurse, a respiratory therapist, a physical therapist, an occupational therapist, a psychologist, and a social worker among others. Additionally breathing games are used to motivate children to perform pulmonary rehabilitation.
Education and training
 Physician performing a bronchoscopy. | |
| Occupation | |
|---|---|
| Names |
|
Occupation type | Specialty |
Activity sectors | Medicine |
| Description | |
Education required |
|
Fields of employment | Hospitals, clinics |
In the United States, pulmonologists are physicians who, after receiving a medical degree (MD or DO), complete residency training in internal medicine, followed by at least two additional years of subspeciality fellowship training in pulmonology. After satisfactorily completing a fellowship in pulmonary medicine, the physician is permitted to take the board certification examination in pulmonary medicine. After passing this exam, the physician is then board certified as a pulmonologist. Most pulmonologists complete three years of combined subspecialty fellowship training in pulmonary medicine and critical care medicine.
Pediatric pulmonologist
In the United States, pediatric pulmonologists are physicians who, after receiving a medical degree (MD or DO), complete residency training in pediatrics, followed by at least three additional years of subspeciality fellowship training in pulmonology.
Scientific research
Pulmonologists are involved in both clinical and basic research of the respiratory system, ranging from the anatomy of the respiratory epithelium to the most effective treatment of pulmonary hypertension. Scientific research also takes place to look for causes and possible treatment in diseases such as pulmonary tuberculosis and lung cancer.
Journals of pulmonology
- American Association for Respiratory Care
- American College of Chest Physicians
- American Lung Association
- American Thoracic Society
- British Thoracic Society
- European Respiratory Society
History of pulmonology
One of the first major discoveries relevant to the field of pulmonology was the discovery of pulmonary circulation. Originally, it was thought that blood reaching the right side of the heart passed through small 'pores' in the septum into the left side to be oxygenated, as theorized by Galen; however, the discovery of pulmonary circulation disproves this theory, which had previously been accepted since the 2nd century. Thirteenth century anatomist and physiologist Ibn Al-Nafis accurately theorized that there was no 'direct' passage between the two sides (ventricles) of the heart. He believed that the blood must have passed through the pulmonary artery, through the lungs, and back into the heart to be pumped around the body. This is believed by many to be the first scientific description of pulmonary circulation.[5]
Although pulmonary medicine only began to evolve as a medical specialty in the 1950s, William Welch and William Osler founded the 'parent' organization of the American Thoracic Society, the National Association for the Study and Prevention of Tuberculosis. The care, treatment, and study of tuberculosis of the lung is recognised as a discipline in its own right, phthisiology. When the specialty did begin to evolve, several discoveries were being made linking the respiratory system and the measurement of arterial blood gases, attracting more and more physicians and researchers to the developing field.[6]
References
^ ACP: Pulmonology: Internal Medicine Subspecialty. Acponline.org. Retrieved on 2011-09-30.
^ Sengupta, Nandini; Sahidullah, Md; Saha, Goutam (August 2016). "Lung sound classification using cepstral-based statistical features". Computers in Biology and Medicine. 75 (1): 118–129. doi:10.1016/j.compbiomed.2016.05.013..mw-parser-output cite.citation{font-style:inherit}.mw-parser-output q{quotes:"""""""'""'"}.mw-parser-output code.cs1-code{color:inherit;background:inherit;border:inherit;padding:inherit}.mw-parser-output .cs1-lock-free a{background:url("//upload.wikimedia.org/wikipedia/commons/thumb/6/65/Lock-green.svg/9px-Lock-green.svg.png")no-repeat;background-position:right .1em center}.mw-parser-output .cs1-lock-limited a,.mw-parser-output .cs1-lock-registration a{background:url("//upload.wikimedia.org/wikipedia/commons/thumb/d/d6/Lock-gray-alt-2.svg/9px-Lock-gray-alt-2.svg.png")no-repeat;background-position:right .1em center}.mw-parser-output .cs1-lock-subscription a{background:url("//upload.wikimedia.org/wikipedia/commons/thumb/a/aa/Lock-red-alt-2.svg/9px-Lock-red-alt-2.svg.png")no-repeat;background-position:right .1em center}.mw-parser-output .cs1-subscription,.mw-parser-output .cs1-registration{color:#555}.mw-parser-output .cs1-subscription span,.mw-parser-output .cs1-registration span{border-bottom:1px dotted;cursor:help}.mw-parser-output .cs1-hidden-error{display:none;font-size:100%}.mw-parser-output .cs1-visible-error{font-size:100%}.mw-parser-output .cs1-subscription,.mw-parser-output .cs1-registration,.mw-parser-output .cs1-format{font-size:95%}.mw-parser-output .cs1-kern-left,.mw-parser-output .cs1-kern-wl-left{padding-left:0.2em}.mw-parser-output .cs1-kern-right,.mw-parser-output .cs1-kern-wl-right{padding-right:0.2em}
^ "Respiratory physiology and sleep sciences".
^ Luis M. Seijo & Daniel H. Sterman (2001). "Interventional Pulmonology". N. Engl. J. Med. 344 (10): 740–49. doi:10.1056/NEJM200103083441007. PMID 11236779.
^ Sharif Kaf A-Ghazal (2002). "The discovery of the pulmonary circulation – who should get the credit: ibn Al-Nafis or William Harvey" (PDF). JISHIM. 2: 46.
^ History of the Division. Hopkinsmedicine.org. Retrieved on 2011-09-30.
Medicine | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||
Specialties and subspecialties |
| ||||||||||||||||||||
| Medical education |
| ||||||||||||||||||||
| Related topics |
| ||||||||||||||||||||
| |||||||||||||||||||||
Authority control |
|
|---|


